Insights
Medical Office Layout Design Guide: Clinic Floor Plans, Exam Room Standards, and Texas Compliance (2026)
May 30, 2026

Medical Office Layout Design Guide: Clinic Floor Plans, Exam Room Standards, and Texas Compliance (2026)
Quick Answer: A compliant Texas medical office layout requires a minimum 80 square feet of clear floor area per exam room (per Texas Department of Health guidelines), dedicated handwashing sinks in every clinical space, ADA-compliant corridors of at least 44 inches, and separation between clean and soiled utility areas. Getting the layout wrong before construction starts is the most expensive mistake a clinic owner can make.
Exam Room Dimensions and Texas Minimum Standards
Texas follows the Guidelines for Design and Construction of Health Care Facilities (the FGI Guidelines) as adopted and amended by the Texas Department of State Health Services (DSHS). For most outpatient medical offices, the minimum clear floor area per exam room is 80 square feet, with no dimension less than 8 feet. This is not a suggestion. DSHS plan reviewers will reject submissions that fall below this threshold.
For comparison, a dentist operatory under Texas State Board of Dental Examiners guidance requires a minimum of 80 square feet as well, but the functional layout differs significantly because dental chairs require a 24-inch clearance on both sides and a 36-inch clearance at the foot of the chair for equipment movement. A general medical exam room can often be arranged in a 10×10 footprint (exactly 100 sq ft) with space for a standard 72-inch exam table, a physician workstation, and a wall-hung sink without feeling cramped. Anything smaller than 10×10 forces compromises that either reduce caregiver reach or push the sink too close to the door.
Procedure rooms need more space. Minor surgical suites, for example, require a minimum of 120 square feet per FGI, and many Texas hospitals and ASCs hold their procedure rooms to 160-200 square feet to allow for equipment carts and additional staff. Imaging rooms are governed by specific radiation shielding requirements from the Texas Medical Board, and those dimensions are set by the equipment manufacturer clearances layered on top of minimum state standards.
| Room Type | Minimum Clear SF | Minimum Clear Dimension | Governing Standard |
|---|---|---|---|
| General Exam Room | 80 sq ft | 8 ft x 10 ft | Texas DSHS / FGI 2022 |
| Dental Operatory | 80 sq ft | 8 ft x 10 ft | Texas SBDE / FGI 2022 |
| Minor Procedure Room | 120 sq ft | 10 ft x 12 ft | FGI 2022 (outpatient) |
| Treatment Room (infusion/PT) | 100 sq ft | 8 ft x 12 ft | FGI 2022 |
| Consultation Room (no exam) | No regulatory minimum | Typically 100-120 sq ft | Practice standard |
Equipment clearances add to minimum room sizes. The standard exam table occupies 24 inches by 72 inches. ADA requires a 36-inch clear path from the door to the foot of the exam table. A wall-hung sink must have at minimum 18 inches of clear space on each side to comply with ADA reach ranges. When you stack all of these clearances against a code-minimum 80-square-foot room, there is essentially zero margin for error. Most experienced designers push exam rooms to 100-110 square feet to give physicians room to move without the layout feeling like a puzzle.
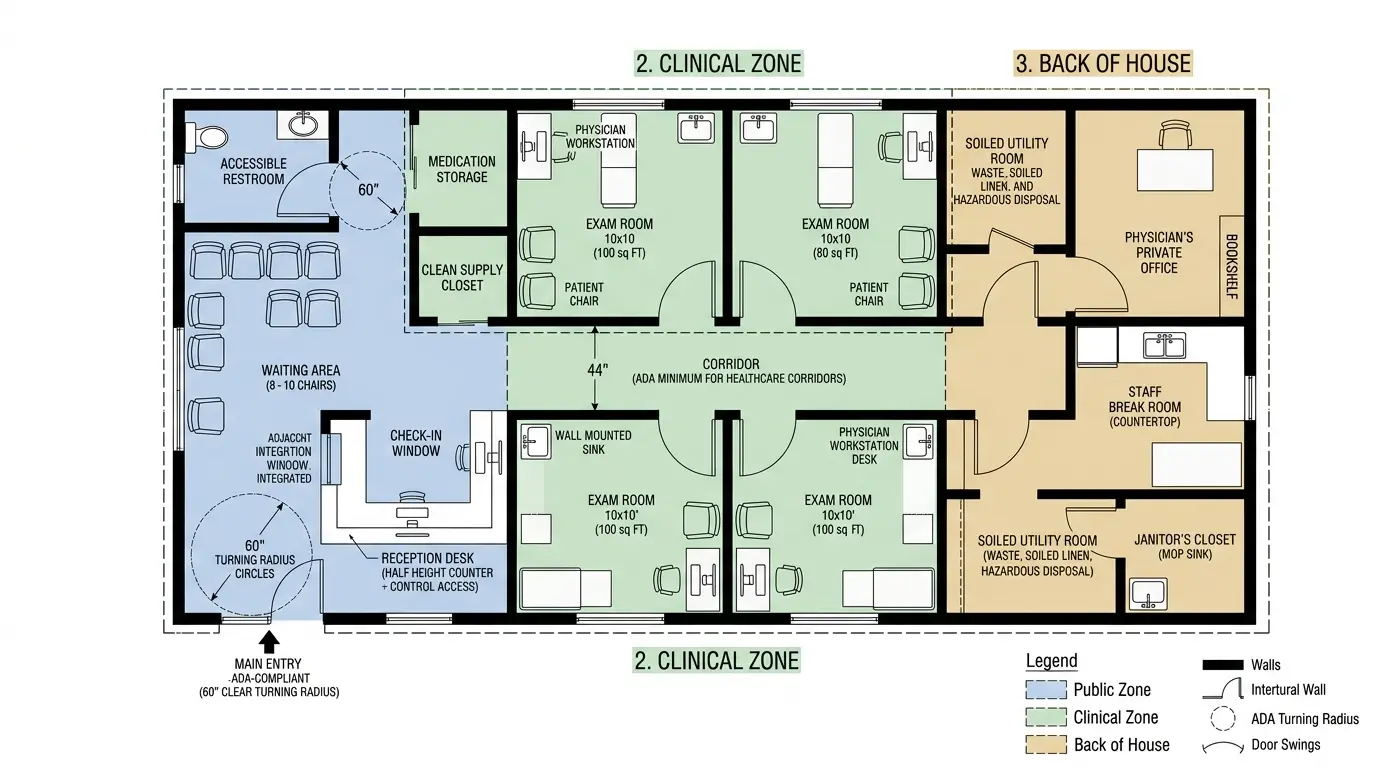
How to Zone a Clinic: Public, Clinical, and Staff Areas
Every functional medical office layout separates the building into three distinct zones: the public zone (lobby, reception, waiting), the clinical zone (exam rooms, procedure rooms, consultation rooms, nurse stations), and the back-of-house staff zone (break room, physician offices, clean and soiled utility). Failing to establish these zones at the planning stage creates HIPAA problems, infection control failures, and workflow inefficiencies that cannot be corrected without tearing out walls.
The public zone should be sized at a minimum of 15 square feet per seat in the waiting area, per DSHS guidance for licensed outpatient facilities. For a 5-exam-room clinic seeing 20-25 patients per day, a waiting room of 200-300 square feet is realistic. The reception desk must have a transaction window or counter that provides a visual separation between the waiting area and the staff work area. HIPAA does not specify exact dimensions, but the HHS Office for Civil Rights expects that incidental disclosures are minimized. A glass partition between the front desk and the waiting room is a common and cost-effective solution.
The clinical zone is the most regulated. Corridors in clinical areas must be at least 44 inches wide per FGI to allow a gurney or wheelchair to pass. Many Texas projects go to 60 inches in primary corridors to allow two people to pass simultaneously without contact. Nurse stations should be positioned to allow line-of-sight to exam room doors so staff can monitor patient movement. In a linear corridor layout (the most common configuration for a small clinic), exam rooms are best arranged on one side of the corridor with storage and utility on the other.
The clean and soiled utility rooms must be physically separated. You cannot store clean supplies in the same space where soiled linens or contaminated instruments are held, even temporarily. Each requires its own locking door. Texas DSHS inspectors check for this specifically in new facility reviews. The soiled utility room must have a service sink (a floor-mounted mop sink or clinical service sink rated for soiled instrument holding) and the clean utility room must have a counter sink with hot and cold water.
Reception-to-Exam Room Ratio: Getting It Right
The most common layout error in small clinic design is underestimating how many exam rooms are needed for the patient volume a provider intends to see. A single physician in a general practice sees an average of 20-24 patients per day on a full schedule. At a 15-minute average visit, that physician cycles through a new exam room every 15 minutes. If the practice uses a traditional “provider-follows-patient” model, two exam rooms per physician is a bare minimum. Most practice consultants recommend 2.5-3 exam rooms per full-time physician for efficient throughput.
| Specialty | Avg Visits/Day per Provider | Recommended Exam Rooms per Provider | Typical Visit Duration |
|---|---|---|---|
| Family Medicine / Primary Care | 20-24 | 3 | 15-20 min |
| Pediatrics | 24-30 | 3-4 | 10-15 min |
| Dermatology | 30-40 | 4-5 | 8-12 min |
| Orthopedics | 20-28 | 3 | 15-20 min |
| Mental Health (therapy) | 6-8 | 1-2 | 45-60 min |
| Dental (general) | 8-12 | 2-3 operatories per dentist | 30-60 min |
The front desk staffing ratio follows from exam room count and patient volume. A single front desk staff member can realistically manage scheduling, check-in, and check-out for a clinic with 3-4 exam rooms. Beyond 4 exam rooms, a second front desk position or a split check-in/check-out counter becomes necessary. The reception desk itself should be designed with enough linear counter space for two simultaneous staff workstations even if you only staff one at opening. Growing into the space is always easier than tearing out casework to add a second station.
ADA Requirements Specific to Medical Offices
Medical offices are Title III places of public accommodation under the Americans with Disabilities Act. This means full ADA compliance is required for all new construction and any alterations that affect primary function areas. Texas also enforces the Texas Accessibility Standards (TAS), which are administered by the Texas Department of Licensing and Regulation (TDLR). TAS is Texas’s adopted version of the ADA Standards and includes some state-specific modifications. TDLR plan review is required for most Texas medical office projects, and a registered accessibility specialist (RAS) must be involved in the design.
Key ADA requirements that affect medical office layout specifically include:
- At least one accessible exam room per specialty per floor, with a 30×60 inch clear floor space alongside the exam table on both sides and the foot
- Accessible height-adjustable exam tables (17-19 inches high in the lowered position) in accessible exam rooms
- Knee clearance under sinks and counters in accessible exam rooms: minimum 27 inches high, 30 inches wide, 19 inches deep
- Door hardware: lever style (not knob) on all patient-accessible doors
- Maneuvering clearance at doors: 18 inches clear on the pull side of all doors in clinical corridors
- Accessible restroom with 60-inch turning radius, grab bars, and compliant fixture heights
TDLR has the authority to require corrections post-construction if plan review or site inspection identifies violations. For a medical office in Texas, budget for a TDLR accessibility review fee (typically $300-$600 for a 2,000-5,000 square foot clinic) and factor the review timeline (4-8 weeks) into your project schedule. Projects that skip this step routinely face stop-work orders or certificate-of-occupancy holds.
For more detail on ADA compliance for Texas commercial spaces, read our guide on ADA requirements for office space in Texas.
HIPAA Privacy Considerations in Physical Layout
HIPAA does not prescribe specific room dimensions or construction details, but the Privacy Rule (45 CFR Part 164) requires covered entities to implement “reasonable safeguards” to limit incidental disclosures of protected health information (PHI). In practice, this translates into specific layout decisions that must be made at the design stage.
The check-in counter is the most common HIPAA layout failure point. If patients can hear the front desk staff verifying insurance, confirming diagnoses, or calling out names across an open waiting room, that is a potential incidental disclosure. Partial-height privacy screens, acoustic baffles, or separate intake consultation windows are the standard architectural solutions. Glass partitions between the front desk and the waiting room are the most cost-effective fix, typically $1,500-$3,000 in materials and labor for a standard reception desk configuration.
Patient sign-in sheets must not be visible to other patients. This is a commonly overlooked detail: a clipboard sign-in sheet sitting on the reception counter that faces the waiting room is a HIPAA concern because patients can read other patients’ names. An angled or recessed counter design eliminates this issue without requiring technology.
Consultation rooms must have acoustic privacy. Standard 3-5/8-inch metal stud walls with a single layer of 5/8-inch gypsum board on each side achieve an STC (Sound Transmission Class) rating of approximately 35-40, which allows clearly audible speech to pass through. For consultation rooms where diagnoses, treatment plans, or mental health discussions occur, an STC of 45-50 is the minimum target. This typically requires full-height walls (to deck, not to drop ceiling), acoustically-rated insulation, and gasketed door frames. Budget $2,000-$4,500 per consultation room for this upgrade over standard wall construction.
Infection Control Zones and Plumbing Requirements
Texas-licensed medical facilities must provide handwashing sinks within each exam room. This is non-negotiable in the DSHS review process. The sink must be accessible to the clinical staff within the room. A sink in a hallway outside the exam room does not satisfy this requirement. Each exam room sink requires a hot and cold water supply, a drain, and ideally a wrist-blade or sensor-operated faucet to prevent contact contamination. Wrist-blade faucets are the lowest cost option at $80-$150 each. Sensor faucets run $150-$350 but are increasingly preferred because they eliminate the touch point entirely.
Plumbing Cost Reality: Adding a sink to an exam room that was not originally designed for one costs $1,800-$4,500 depending on how far the drain must run to connect to the main waste stack. In a single-story slab-on-grade building (common in suburban Texas), cutting the slab to run drain lines is the primary cost driver. This is why getting the layout right before construction is critical. Moving a sink on paper costs nothing. Moving a sink after the slab is poured costs $3,000-$6,000.
Instrument reprocessing (sterilization) areas require their own dedicated zone separate from both patient care and clean supply storage. A basic autoclave station needs a minimum of 6 linear feet of counter space, a sink, and adequate ventilation to exhaust heat from the sterilization cycle. The soiled side (instrument receiving and pre-cleaning) must be physically separated from the clean side (sterile storage) either by a pass-through window or by separate rooms. Texas DSHS inspectors follow CDC and OSHA instrument reprocessing guidelines and will flag any configuration that allows clean and soiled instruments to cross paths.
Janitors’ closets and mop sinks in clinical areas must be located to prevent cross-contamination. The mop sink should never share a space with clean supply storage. In small clinics where space is limited, a dedicated 40-square-foot janitor’s closet with a floor-mounted service sink is the minimum acceptable configuration.
Texas DSHS Requirements for New Medical Facilities
The Texas Department of State Health Services regulates healthcare facility construction through the Health Facility Licensing division. Any new outpatient clinic, ambulatory surgery center, birthing center, or imaging center in Texas must submit architectural plans to DSHS for review before construction begins. This is separate from the city or county building permit process. You need both approvals.
The DSHS plan review process for a new outpatient clinic typically takes 8-12 weeks for an initial review cycle. If the reviewer issues deficiencies (which is common on first submission), you have 30 days to respond. Each subsequent review cycle adds 4-6 weeks. Plan on 4-6 months from design completion to DSHS approval for a project without unusual complications. Projects in Austin, San Antonio, and Houston often experience longer review times due to volume.
The plans required for DSHS submission include architectural floor plans, reflected ceiling plans, plumbing plans, mechanical plans, and a written narrative describing the scope of services and patient population. DSHS uses the 2022 FGI Guidelines as its primary reference document, supplemented by the Texas Administrative Code (25 TAC Chapter 135 for ambulatory surgical centers, Chapter 133 for hospitals). For most small outpatient medical offices, the applicable code is DSHS’s general outpatient facility standards, which are less prescriptive than hospital or ASC codes but still require professional plan preparation.
Key Point on Physician Office Exemptions: A “physician’s office” that provides only routine outpatient care and does not perform invasive procedures may be exempt from DSHS facility licensing under certain conditions. However, this exemption is narrow. If your clinic will perform any procedure requiring sedation, conduct imaging with ionizing radiation, or operate as a multi-specialty group practice under a non-physician management structure, consult a healthcare attorney before assuming the exemption applies. The cost of a licensing compliance review ($1,500-$3,000) is far less than the cost of a stop-work order or post-construction modification requirement.
Texas also requires that healthcare facilities file a Notice of Intent (NOI) with DSHS before construction begins. The NOI is a simple form but triggers the formal plan review clock. Missing this step can result in fines and delays if discovered during inspection.
What We See in Texas Medical Office Projects
We work on medical office tenant improvements and ground-up clinic designs across San Antonio, Austin, and the Hill Country. Here is what we consistently encounter on these projects.
The most expensive mistake we see is a physician who leased space before engaging a designer. They signed a 5-year lease on 2,400 square feet, paid a construction cost to build out 4 exam rooms, and then discovered that the slab-on-grade floor requires core drilling to add the required exam room sinks. Three of the four exam rooms were positioned over the structural thickened-edge slab where drilling is not feasible without structural engineering review. The project budget grew by $28,000 to relocate two exam rooms and add plumbing infrastructure. A pre-lease space assessment by a designer who understands medical plumbing requirements would have cost $2,000-$3,500 and would have identified this issue before the lease was signed.
We also see undersized waiting rooms routinely. A physician who projects 15 patients per day often grows to 22-25 within 18 months of opening. A waiting room designed for 8 patients feels crowded with 14. Designing for growth at the outset adds very little cost because you are simply allocating more square footage to waiting versus exam rooms. The cost to reconfigure a waiting room after construction is $15,000-$40,000 depending on whether walls need to be moved.
Acoustic privacy is the most commonly skipped upgrade. Standard partition walls between exam rooms are rarely built to STC 45. Patients in adjacent exam rooms can hear each other clearly. We have seen this become a patient retention issue for practices in competitive markets where the patient experience matters. Building acoustic walls costs $8-$12 per square foot more than standard walls. On a 100-square-foot exam room with two shared walls, that is $1,600-$2,400 per room. Worth every dollar.
Typical Cost Ranges by Room Type
| Room Type | Typical Size (sq ft) | Construction Cost Range | Notes |
|---|---|---|---|
| Standard Exam Room | 100-120 | $18,000-$30,000 | Includes sink, exam table alcove, casework, tile floor |
| Procedure / Minor Surgery Room | 150-200 | $35,000-$60,000 | Includes upgraded lighting, LVT floor, additional electrical |
| Reception / Front Desk Area | 150-200 | $25,000-$45,000 | Includes custom millwork, privacy glass, IT infrastructure |
| Waiting Room | 200-400 | $12,000-$22,000 | Furniture not included; includes flooring, lighting, finishes |
| Clean / Soiled Utility | 60-100 each | $12,000-$20,000 per room | Includes service sink, casework, ventilation |
| Sterilization / Reprocessing Area | 80-120 | $18,000-$32,000 | Pass-through window, dedicated exhaust, specialty countertop |
These ranges reflect general contractor pricing in the San Antonio and Austin metro markets for tenant improvement work in existing commercial buildings. Ground-up construction adds 20-35% to these figures due to site work, foundation, and shell costs. Projects in Hill Country markets (Boerne, Kerrville, Fredericksburg) may see 10-15% higher labor costs due to contractor availability. For more context on tenant improvement budgeting, read our guide on tenant improvement costs per square foot in Texas.
Key Takeaways
- Texas DSHS requires a minimum 80 square feet of clear floor area per exam room. No dimension can be less than 8 feet.
- Every exam room must have a handwashing sink within the room. A hallway sink does not satisfy DSHS requirements.
- Plan for 2.5-3 exam rooms per full-time physician to avoid throughput bottlenecks.
- Clean and soiled utility areas must be physically separated with individual locking doors.
- DSHS plan review for a new outpatient clinic typically takes 4-6 months total. Factor this into your project schedule before signing a lease.
- HIPAA layout requirements affect the front desk, consultation rooms, and sign-in process. Address them at the design stage, not after occupancy.
- Acoustic privacy in exam rooms and consultation rooms requires full-height walls and STC 45+ construction. Standard partition walls do not achieve this.
- Moving a sink after the slab is poured costs $3,000-$6,000. Get the layout right before construction starts.
Frequently Asked Questions
What is the minimum size for a medical exam room in Texas?
Texas requires a minimum of 80 square feet of clear floor area per exam room, with no single dimension less than 8 feet, per the Texas Department of State Health Services standards based on the FGI Guidelines for Design and Construction of Health Care Facilities (2022 edition). This is the code minimum. Most designers recommend 100-120 square feet to provide adequate clearance for ADA-compliant exam tables, physician workstations, and handwashing sinks without feeling cramped.
Does a medical office in Texas need DSHS plan review?
Most licensed healthcare facilities in Texas, including outpatient clinics, ambulatory surgery centers, and imaging centers, require DSHS plan review before construction begins. A narrow exemption exists for physician offices providing only routine outpatient care without invasive procedures or sedation, but this exemption is easy to misapply. Budget 4-6 months for the DSHS review and approval process, and engage a healthcare designer familiar with the Texas submission requirements to minimize review cycles.
How much does it cost to build out a medical exam room in Texas?
A standard medical exam room in San Antonio or Austin runs $18,000-$30,000 to build out in an existing commercial space, including the required sink, exam table alcove, casework, tile or LVT flooring, and finishes. Procedure rooms run $35,000-$60,000 due to upgraded lighting, additional plumbing, and specialized flooring. These figures reflect 2026 general contractor pricing for tenant improvement work and do not include equipment or furniture.
What are the HIPAA layout requirements for a medical office?
HIPAA’s Privacy Rule does not specify exact room dimensions but requires “reasonable safeguards” to limit incidental disclosures of protected health information. In practice, this means: (1) a reception desk with a privacy partition between staff and the waiting room, (2) consultation rooms with acoustic wall construction achieving STC 45 or higher, (3) a sign-in process that does not expose other patients’ names, and (4) corridors that do not route patients through staff work areas where PHI may be visible on screens or documents.
Ready to Design Your Texas Medical Office?
Prestige 360 Design specializes in medical office tenant improvements and clinic buildouts across San Antonio, Austin, and the Texas Hill Country. We handle the full scope from pre-lease space assessment through DSHS plan submission and construction administration, so you open on time and in compliance.
Schedule a consultation with our team to review your space and discuss your clinical program before you sign a lease or hire a contractor.